VA uses diagnostic code 6260 for tinnitus, which provides a 10 percent rating for recurrent tinnitus. In some circumstances, VA may also assign a 0 percent rating for non-recurrent tinnitus (although VA may also simply deny service connection in such a scenario). 10 percent is the highest rating that may be assigned for tinnitus.
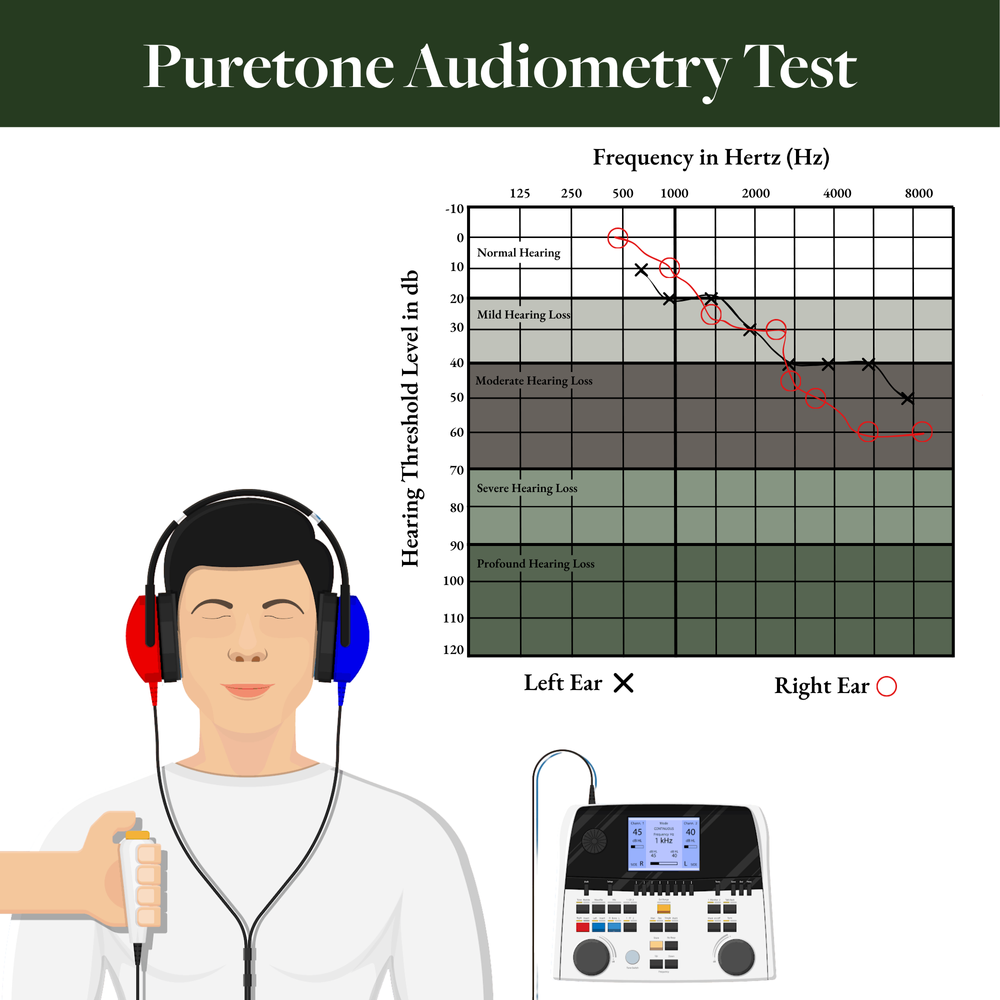
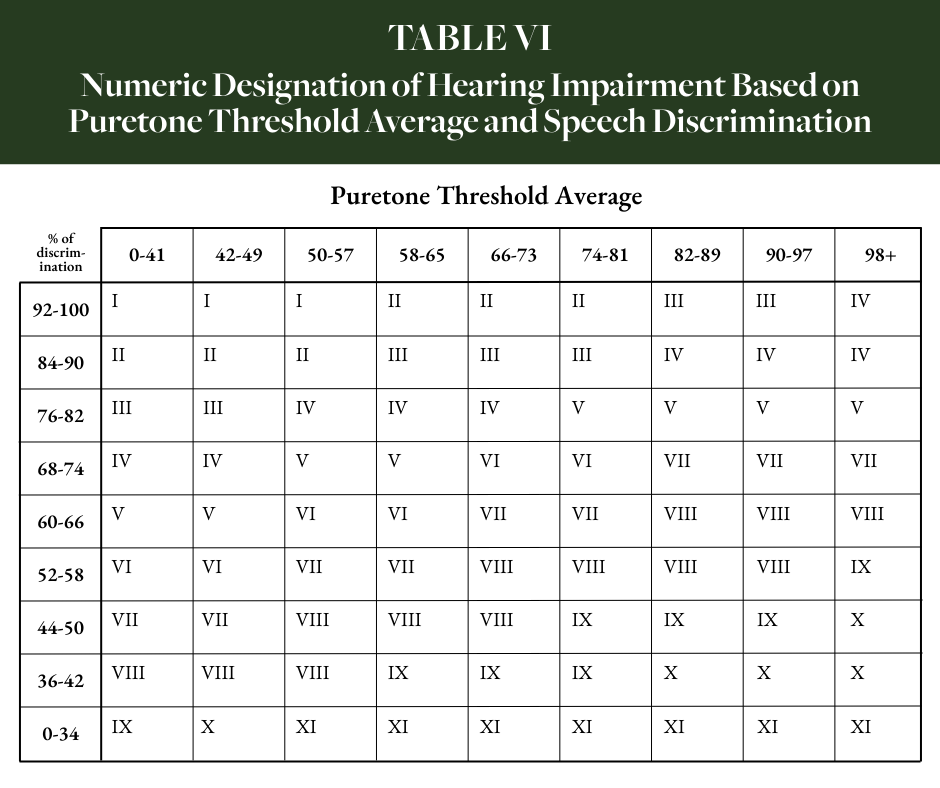
VA rates hearing loss using multiple tables provided in 38 C.F.R. § 4.85 to combine the Puretone threshold average and percent of speech discrimination values for each ear and then to combine those of each ear. First, VA uses Table IV to identify the Roman numeral corresponding to the combination of Puretone threshold average and speech discrimination percentage. If rating solely on Puretone threshold average, then Table IVA is used instead. Once the appropriate Roman numeral for each ear has been identified (if only service-connected in one ear, then the non-service-connected ear is assigned a Roman numeral value of I for rating purposes), Table VII is used to identify the corresponding rating for the combination of both Roman numerals, with the better ear represented in the vertical rows and poorer ear in the horizontal columns.